Vitamin D – essential to good health




This column is written by Stig Bengmark – professor emeritus, researcher, lecturer and author. Read more of Stig’s columns here.
Vitamin D deficiency – a misery with no equal
The history of vitamin D deficiency is long and full of indescribable agony. Here in Sweden, both children (from 6 months and up) and adults have historically suffered from vitamin D deficiency to an incredibly extensive extent – that was the price you had to pay for living so far north. Vitamin D deficiency was particularly widespread in the 1600s-1700s, which was probably related to the fact that the population moved to cities to a greater extent.
The condition was first described in the medical literature around 1750 by, as was so often the case at the time, two English doctors. The condition was renamed rickets across the rest of the world, but was named the engelska sjukan (English disease) in Sweden. The disease typically started with severe digestive problems and, in children, indescribable crying – as soon as the mothers touched their children they cried out in pain. Vitamin D deficiency resulted in soft bones, and if not treated in time, permanent bone deformities – severe deformities led to serious disabilities and made it difficult for women to bear children. Extensive damage to teeth and premature tooth loss were also common and occurred in a large section of the population.
There was no real treatment for the condition until around 1920 when the condition was first explained – a deficiency of vitamin D. The English scientist Edward Mellanby, who was just 35 at the time, was the first to identify the condition created by vitamin D deficiency as the explanation for the onset of rickets. Experimental dogs that lived solely on a diet of porridge developed a vitamin D deficiency fairly quickly, but could be cured by adding fish liver oil to the porridge. Edward’s wife May Mellanby would later show that vitamin D has an extensive ability to prevent and heal dental damage, which has been a tremendous benefit to humanity. Over the long term, the vitamin D discovery will certainly come to mean much, much more – especially with penicillin slowly coming to the end of its lifespan while the benefits of vitamin D are only beginning to be revealed.
Vitamin D is much more than a vitamin – it regulates hundreds of important processes in the body
Vitamin D is not like any other vitamin we have come to know over the last 100 years, it is also an important hormone and, above all, a crucial factor for healthy, well-functioning gut flora and the proper function of the immune system – properties that we have only recently begun to examine more closely.
For many years, the primary interest in vitamin D centred around its ability to support bone formation, the absorption of minerals such as calcium and magnesium leading to mineralization in the bones, and its ability to prevent rickets in children and osteoporosis in the elderly. Only a relatively small amount of added vitamin D is needed to support these functions, which explains why the recommended daily dose for children and adults has long been kept at a low level. But to maintain healthy, well-functioning gut flora and an optimal immune response, it appears that much higher levels of vitamin D are needed in the body!
Rare at the equator – very common in the Nordic countries
The further one lives from the equator, the more likely you are to have vitamin D deficiency – that is the price we pay for living so far north. In Sweden, mild vitamin D deficiency is the rule rather than the exception, and it has been found that more than 80% of children and adolescents in Upper Norrland and more than 60% in southern Sweden (Gothenburg) have documented vitamin D deficiency. But despite the favourable conditions at the equator, vitamin D deficiency is now also being seen there – dark-skinned people need 4 to 5 times more sun exposure than light-skinned people to absorb vitamin D, and there are often religious restrictions in these countries that require one to cover one’s body, especially women. This has also created a major problem in Sweden as well – dark-skinned people have significantly increased morbidity in Sweden than light-skinned people. in countries at or near the equator, diseases such as asthma, type 1 diabetes, inflammatory bowel disease and multiple sclerosis are very rare.
Mother Sun provides – diet is not the only thing that can help here
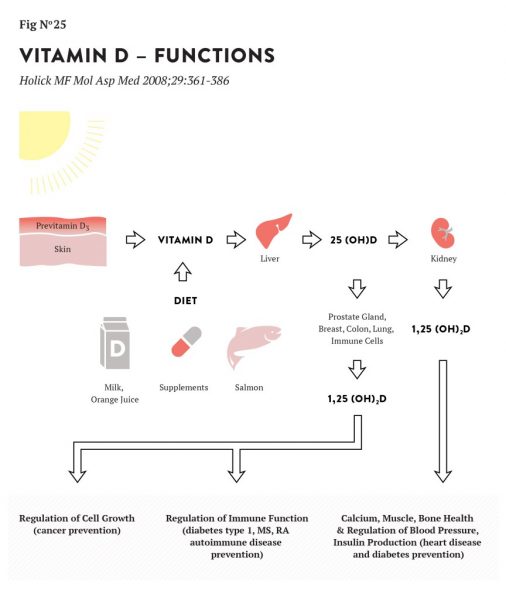
The parathyroid, brain, kidneys, intestines, gut flora and skeletal system are particularly sensitive to low vitamin D levels. And the body’s need for vitamin D cannot be met by diet alone. The primary food sources of vitamin D are fatty fish, eggs and whole milk, but the amount of vitamin D you can get from such a diet is simply not enough – no one can eat the sheer quantity of oily fish and eggs that would be needed to get enough vitamin D. There is only one, all natural remedy that takes care of the need for Vitamin D – go out in the sun and expose your skin. The sun’s job is to convert a precursor (cholesterol) in the skin into vitamin D, which is typically stored in the body for future needs. Given how far Sweden is from the equator, this can only happen during the summer months.
During the winter months, no new vitamin D is synthesised and the vitamin D your body has stored quickly thins out – for every 6-week period after September, our body’s vitamin D stores decrease by half. This means that the body’s stores are running extremely thin by the time March-April comes along – a period when new diseases often debut and others return, including depression and inflammatory bowel diseases.
Sunbathing, especially in the middle of summer, is extremely effective. One hour of full-body sunbathing in the middle of the day provides about 24,000 IU of vitamin D – just 10-15 minutes of sun is enough to supply the body with Vitamin D for several days. It is partly a misconception that we should avoid sunbathing in the middle of the day – that is exactly when you should sunbathe – but do it carefully and avoid sunburn!
The sun actually has two different kinds of “rays”, harmful/carcinogenic UV-1 rays and UV-2 rays, which are beneficial for the body’s vitamin D needs. The ratio between the beneficial/harmful UV rays is at its best in the middle of the day. It is therefore better to sunbathe for a short time in the middle of the day than for a longer time earlier or later in the day – you are still exposed to some of the sun’s harmful rays, but you are able to get much more of the sun’s beneficial rays!
Vitamin D deficiency contributes to many diseases – almost ALL of them
Vitamin D deficiency has been shown to be related to a vast array of health conditions, including: allergies, Alzheimer’s disease, asthma, autism, sepsis, cancer, Crohn’s disease, cystic fibrosis, macular degeneration, depression, diabetes 1 and 2, poor hearing, poor sports performance, eczema, epilepsy, obesity , colds, premature aging, complications in pregnancy and childbirth, heart disease, tooth decay, high blood pressure, infection, infertility, influenza, lung diseases including COPD, migraines, multiple sclerosis, muscle pain, oral diseases such as gingivitis, caries and tooth loss, kidney disease, Parkinson’s disease, psoriasis and other skin conditions, rheumatic diseases, schizophrenia, tuberculosis and vaginal discharge.
Vitamin D deficiency does not necessarily have to be present at the exact moment an illness debuts, both Multiple Sclerosis and Parkinson’s disease, for example, have been strongly linked with periods of vitamin D deficiency at earlier stages in life. Studies show that the majority of people who come to the hospital with chronic diseases have vitamin D deficiency – e.g. those who come in for surgery due to various chronic diseases: obesity surgery 57% (dark-skinned people 79%), kidney transplant 67% (dark-skinned people 95%), chronic pancreatitis surgery 77% and hip/knee replacement 85%. It would certainly be very interesting to know how many of these treatments/surgeries could have been avoided if we had considered the need for vitamin D earlier on in life.
The ability of vitamin D to prevent influenza and other seasonal infectious diseases is phenomenal

It is certain that major flu epidemics in the past, such as the Spanish flu, for example, took millions of lives because most countries had more or less widespread vitamin D deficiency. It is especially important to know that in several studies, vitamin D, probiotics and synbiotics have also been shown to have a phenomenal ability to stave off infection and influenza that so frequently affects the population in the spring when vitamin D levels in the body are at their lowest. In fact, there is no medicine available that can compete with vitamin D in this respect.
In one study, 25% of those who did not receive a vitamin D supplement developed the flu in the winter months, while only 3% of those who received 800 IU (20 µg) of vitamin D per day got the flu. And those who received 2000 IU (50 µg) per day showed no flu whatsoever.
Regular vitamin D supplementation dramatically reduces morbidity and saves society billions
If all the people living in Europe consistently maintained normal vitamin D levels, the frequency of a number of diseases would decrease dramatically. A joint US/European research project (Gant WB et al. Prog Biophys Mol Biol 2009;99:104-113) used a methodology developed by Professor Emeritus of Health Economics Bengt Jönsson at the Stockholm School of Economics to identify what effects it would have if it was ensured that all EU residents had normal vitamin D levels in their blood at all times. They set the cut-off point for vitamin D deficiency at a very low level (40 ng/mL), but most researchers today, even public health agencies in some countries, agree that it should be almost twice that amount (70 ng/mL). In most cases, 40 ng/mL is reached with a daily intake of 2000-3000 IU (50-75 µg) of vitamin D, and the cost of reaching that level (information, testing, cost of vitamin D, etc.) is estimated to be EUR 10 million per year (about SEK 95 million). On the other hand, the gains (reduced cost of morbidity/health care) are estimated to be no less than EUR 187 billion/year (approximately SEK 1.765 billion) – which corresponds to 36% of all indirect healthcare costs in the EU and 28% of direct costs.
This would amount to a huge reduction in disease: one estimate is that cardiovascular disease (mostly heart attacks and strokes) would decrease by up to 14%, infectious diseases including influenza by up to 7%, type 2 diabetes by up to 7%, cancer by up to 6.4%, osteoporosis by about 1.5% and multiple sclerosis by at least 1%. So there is a lot of evidence that your gut flora and immune system would benefit from a higher level of vitamin D in the body – at this point, we can only speculate on the hopefully even greater gains that could be made if we had set the ideal deficiency cut-off point at 70 ng/mL
It is high time that we put this knowledge to use
One would think that such valuable information would create a feverish level of activity among Europe’s health policy makers, but this has not been the case in the past, nor is it today. It automatically makes you think of Alf Henrikson’s poem:
“It was what it was, until it became what it became (translation from original Swedish).
It will be what it is, while it is as it is.
It is what it is, until it becomes what it becomes.
The danger is that it will be what it was”.
Many years ago, I was a member of a government commission (the 1969 Open Health Care Commission), one of the investigations that preceded the construction of hundreds of health care centres across the country. In the commission’s report, we argued that one of the most important tasks of the health care centres would be to provide information about health, educate the public about health and work actively with preventive measures. Hundred of health care centres were built, but no preventive measures were implemented -and that is still the case today. For example, no county will pay for the cost of a vitamin D test today unless there are symptoms of a vitamin D deficiency.
What level of vitamin D should one strive for?
Studies that were recently published showed that Africans living in rural settings have a vitamin D level of between 115 and 125 ng/mL – thus a much higher level than we see in northern Europe. The EU’s specially appointed Scientific Committee recommends an intake of up to 50 µg (2000 IE, 1 µg = 40 IE) as an upper daily limit for adults and 25 µg (1000 IU) for children.
The fact that there are so many individual differences also presents a major problem. For example, I have met athletes who closely monitor their vitamin D values by regularly having US laboratories analyse their vitamin D levels, and they have told me that despite taking 10,000 IU (250 µg), they have a really hard time getting their levels over 70 ng/mL. Absorption is improved if you consume some form of fat with the vitamin D, but it does not solve the problem completely. Researchers agree that older people with thinner skin have a decreased ability to synthesise vitamin D and also lower absorption rates, and therefore need a larger dose – certainly double that. My wife and I take 5000 IU (125 µg) of vitamin D per day all year, which gets me to a level of just over 80 ng/mL, while my slightly younger wife reaches the “African” level at just over 120 ng/mL.
What if our health care centres could get the resources they need to test vitamin D levels? I often promote the importance of preventative health care to prevent expensive health care. All I can do is keep pestering them and hope that our politicians one day recognise the kind of savings that can be made. Providing the opportunity for vitamin D testing is an excellent example.